“The model enabled precise and anticipatory visualization of the tumor’s relationship with vascular and visceral structures, facilitating a safer, targeted oncologic surgery tailored to the patient’s real anatomy”.

Dr. Antonio Melero Abellán, Consultant, Accredited Unit of Colorectal and Robotic Surgery, Department of General and Digestive Surgery, Hospital General Universitario de Valencia
Case Presentation
A 49-year-old male patient was referred from a Specialty Care Center following a colonoscopy performed at a private institution diagnosing colon neoplasia. For the past year, he had experienced central abdominal pain and rectal bleeding, with progressive worsening, along with weight loss and anorexia in the previous month. He had no relevant personal or family medical history.
Complete colonoscopy revealed a tumor occupying two-thirds of the colonic circumference, with an ultrashort traction pseudopolyp. The lesion was superficial and firm. Biopsies were obtained, and the lesion was tattooed with India ink 2 cm distally.
Histopathological analysis confirmed mucinous (colloid-type) adenocarcinoma. Immunohistochemistry demonstrated loss of MSH6 expression, with preserved MSH2 and PMS2 expression.
Contrast-enhanced thoracoabdominopelvic CT showed colocolic intussusception at the descending colon level, mesenteric lymphadenopathy, and adjacent fat stranding, suggestive of a neoplastic process. Radiologic staging was T3 N+, with at least seven suspicious locoregional lymph nodes.
The case was reviewed by the Multidisciplinary Colorectal Tumor Board, and upfront surgery was indicated without neoadjuvant oncologic treatment. A laparoscopic oncologic segmental resection of the splenic flexure / left hemicolectomy was proposed. Personalized 3D surgical planning using the CELLA model was requested.
Within the prehabilitation protocol (GRAMGEA), mild Factor VII deficiency was detected and assessed by Hematology, with preoperative vitamin K supplementation indicated.
The patient weighed 80 kg, measured 177 cm (BMI 25), and was classified as ASA I. He received a 1500 mg intravenous iron bolus and was instructed in respiratory physiotherapy exercises.
In the operating room, a patient-specific, navigable 3D virtual model based on imaging studies was available throughout the procedure, enabling a directed, precise, and personalized surgical approach.
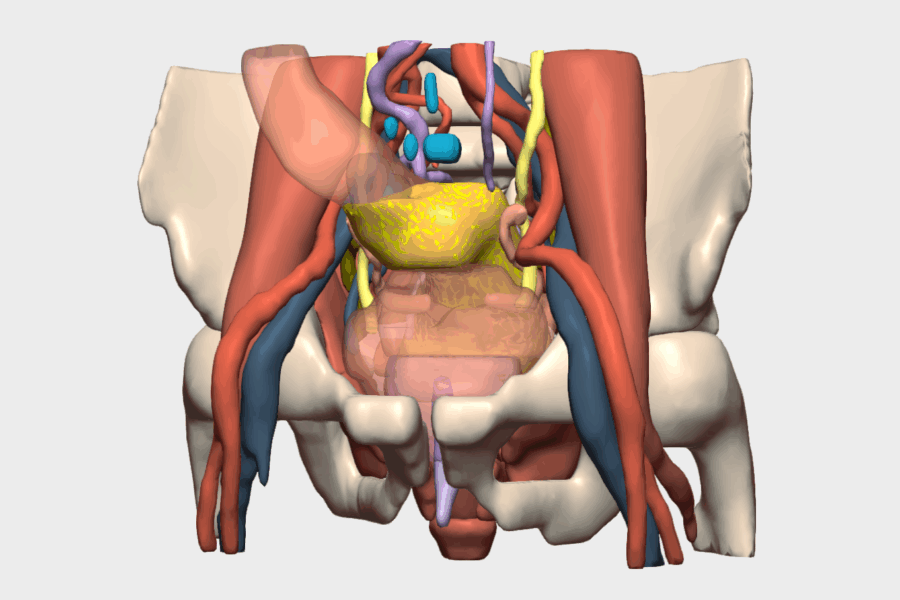
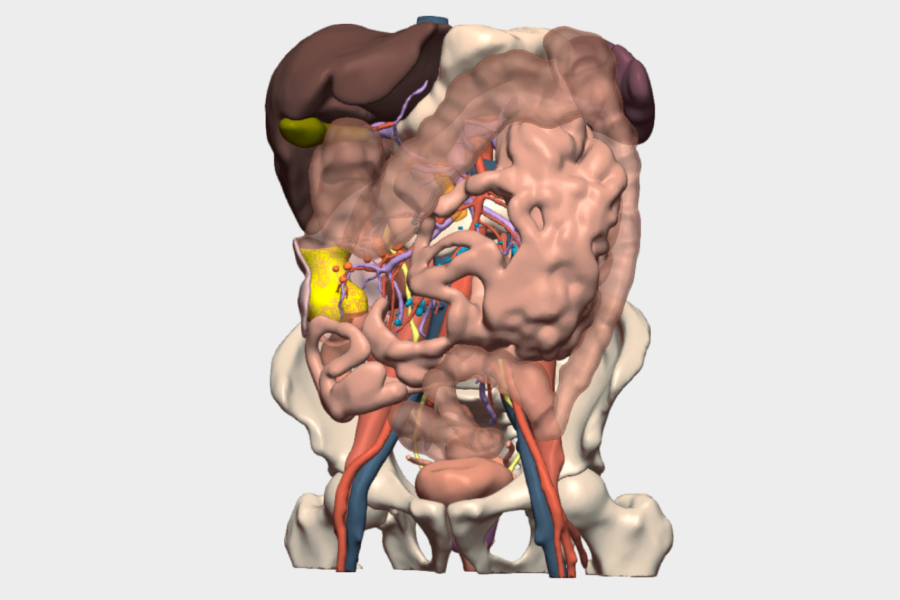
The tumor was identified at the splenic flexure, presenting significant induration, neovascularization, and colocolic intussusception, findings consistent with the 3D model. The inferior mesenteric vein (IMV) was identified, and mesocolic dissection was performed while preserving the pancreatic tail, spleen, and left Toldt’s fascia.
Thanks to the 3D reconstruction, two left colic arteries arising directly from the aorta were identified, in addition to the left colic trunk originating from the inferior mesenteric artery (IMA). This anatomical information enabled selective vascular ligation, preserving the inferior mesenteric artery and the more distal left colic artery, which was not involved with the tumor nor within the oncologic safety margins. This strategy optimized the segmental resection of the splenic flexure. The left branch of the middle colic artery was also divided.
Due to technical difficulty performing an intracorporeal anastomosis, a mechanical side-to-side colocolic anastomosis was performed, with intraoperative perfusion assessment using indocyanine green (ICG).
The postoperative course was favorable, with minimal intraoperative blood loss (approximately 25 cc). The patient experienced a transient episode of acute confusional syndrome on postoperative day two, which resolved completely within 24 hours. He was discharged on postoperative day three without complications.
Final histopathological analysis confirmed a moderately differentiated mucinous (colloid-type) adenocarcinoma, with mesocolic invasion greater than 5 mm and a 2 mm nodal metastasis in 1 of 25 lymph nodes examined. Final staging: pT3N1a (AJCC 8th edition).
Surgical Planning with a 3D Model
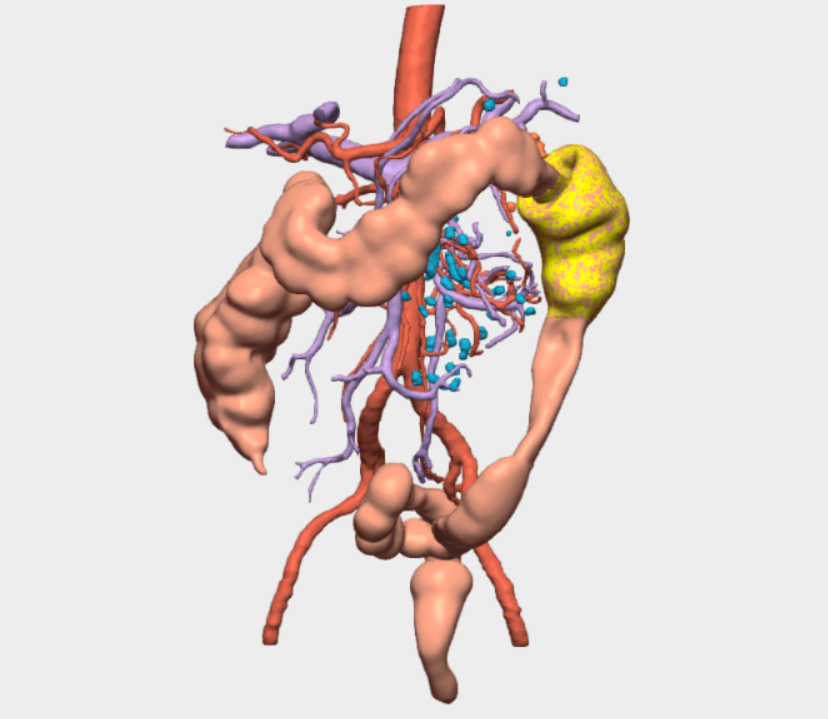
The 3D reconstruction was particularly relevant for the identification and comprehensive understanding of the mesenteric vascular anatomy, revealing the presence of two left colic arteries—an anatomical variant with direct impact on surgical strategy.
It also enabled precise anticipation of the tumor’s location at the splenic flexure, its relationship with the colocolic intussusception, and its proximity to critical structures such as the pancreas and spleen, thereby reducing intraoperative uncertainty and enhancing procedural safety.
The CELLA 3D model provided real-time, interactive, and navigable visualization, with detailed segmentation of vessels, colon, mesocolon, and adjacent organs. The ability to rotate the model, isolate specific structures, and correlate the virtual reconstruction with real intraoperative anatomy was essential for accurate vascular identification and safe resection planning.
This functionality offered significant added value by facilitating a more predictable, personalized, and efficient surgical approach, resulting in minimal blood loss and an excellent postoperative course.

Surgical Outcome
The procedure was successfully completed using a laparoscopic approach, achieving an adequate and personalized oncologic resection with selective vascular ligation guided by 3D planning. The surgery proceeded safely, with minimal blood loss, no intraoperative complications, and excellent anatomical control in a highly complex area such as the splenic flexure.
The postoperative course was favorable, allowing for early recovery and hospital discharge without significant surgical complications. The CELLA 3D surgical planning model was a key element in anticipating the patient’s individual vascular anatomy, reducing intraoperative uncertainty, and supporting real-time decision-making. This contributed to a more precise, predictable, and safer surgical procedure.
This case exemplifies the value of 3D reconstruction as a fundamental tool in complex, personalized colorectal surgery, enhancing quality of care and improving clinical outcomes.
The surgery was performed by Dr. Antonio Melero Abellán, Consultant in the Accredited Unit of Colorectal and Robotic Surgery, Department of General and Digestive Surgery, Hospital General Universitario de Valencia, together with Dr. Fernando Alfonso García, third-year resident in General and Digestive Surgery at the same institution.
¡Follow us on social media to stay up to date with our latest updates.!