
”The 3D model enabled us to achieve a radical resection while minimising postoperative sequelae”.
Dra. Carmen Benlloch, Paediatric Surgeon, Hospital Clínico Universitario de Valencia
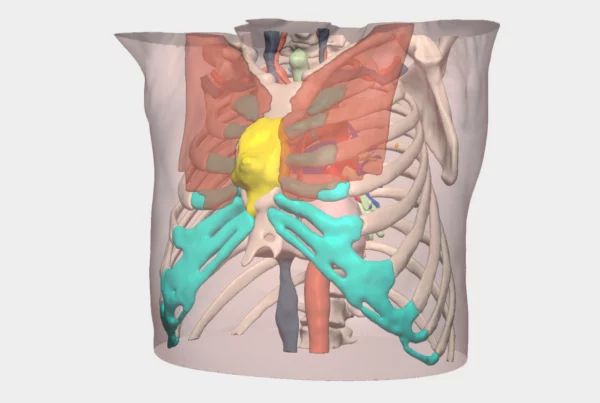
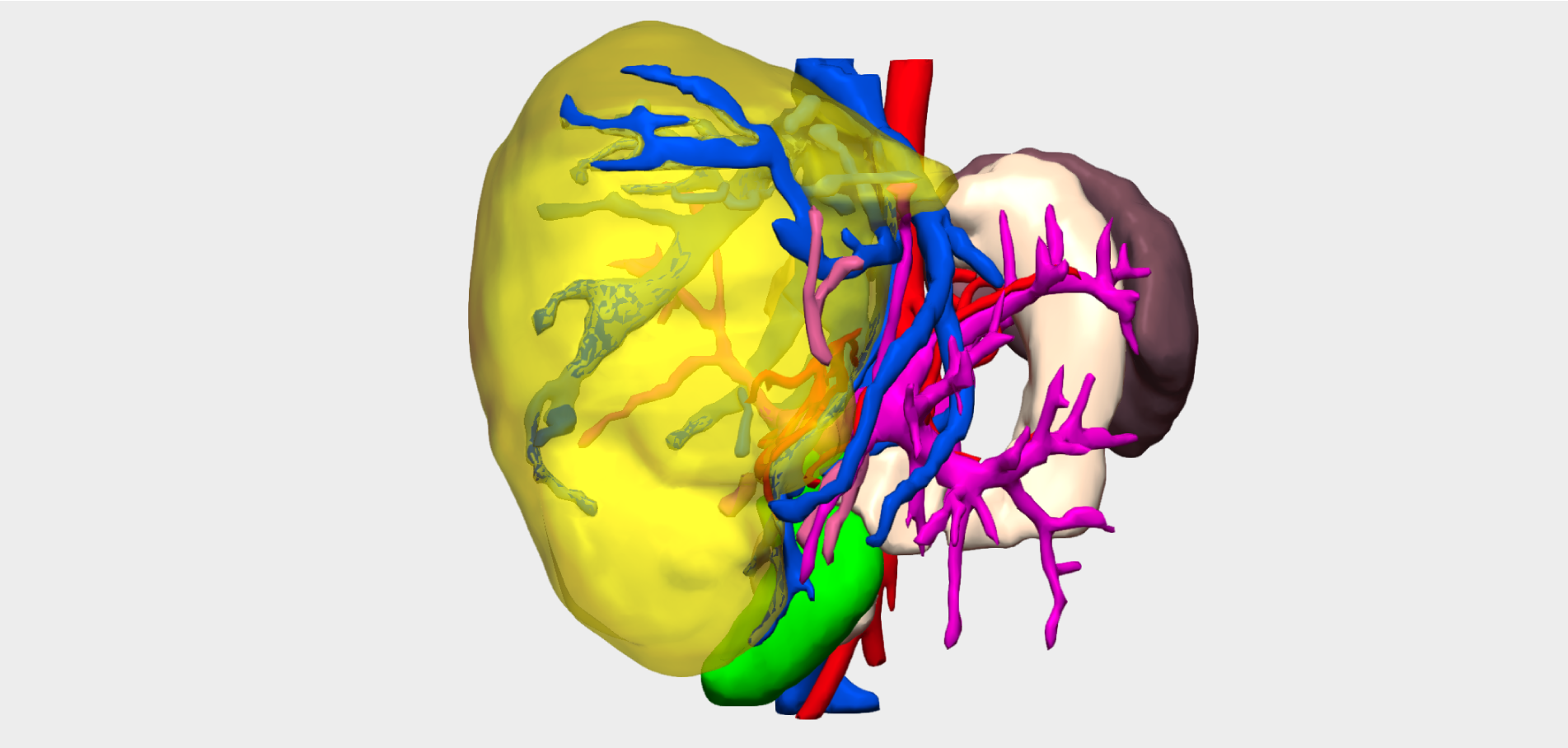
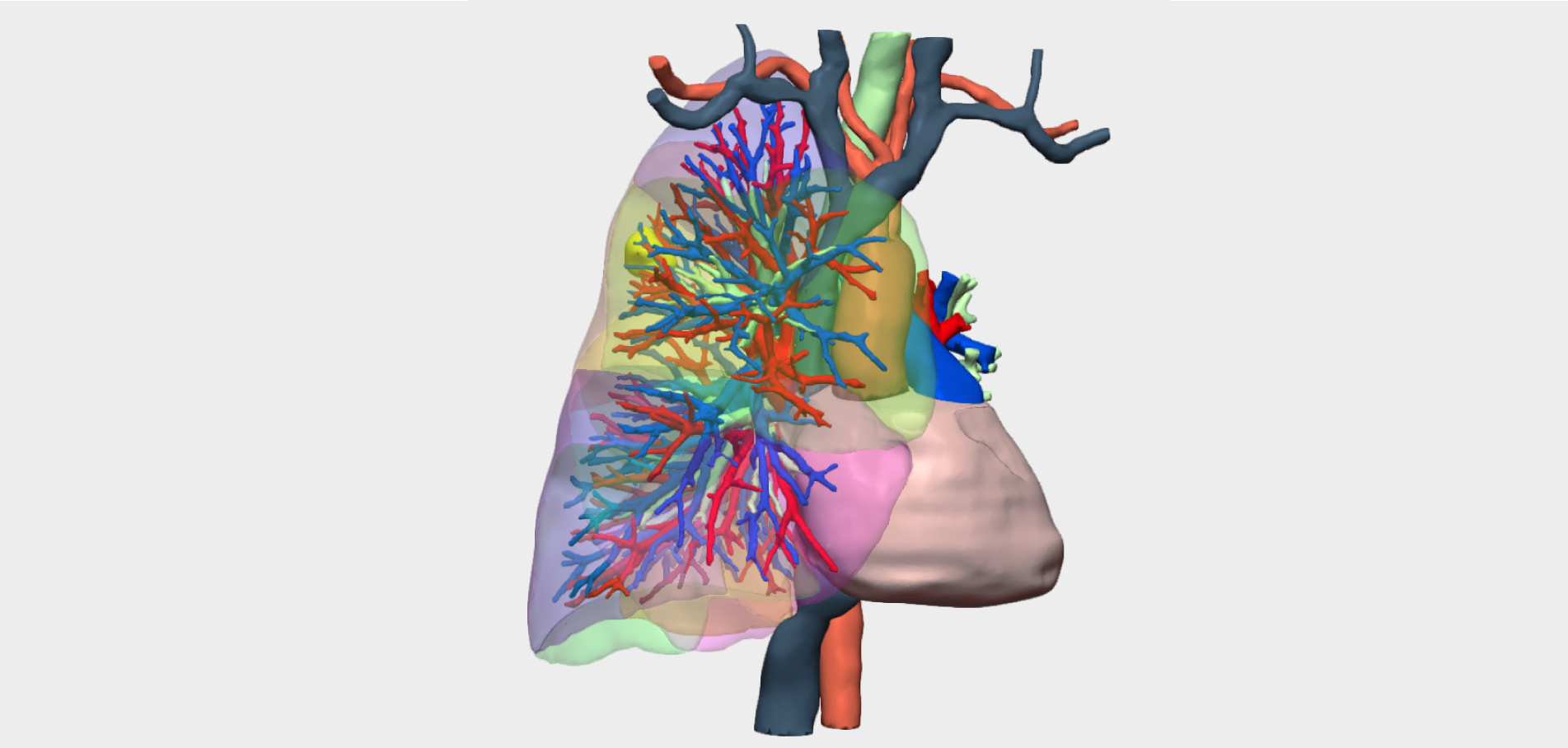
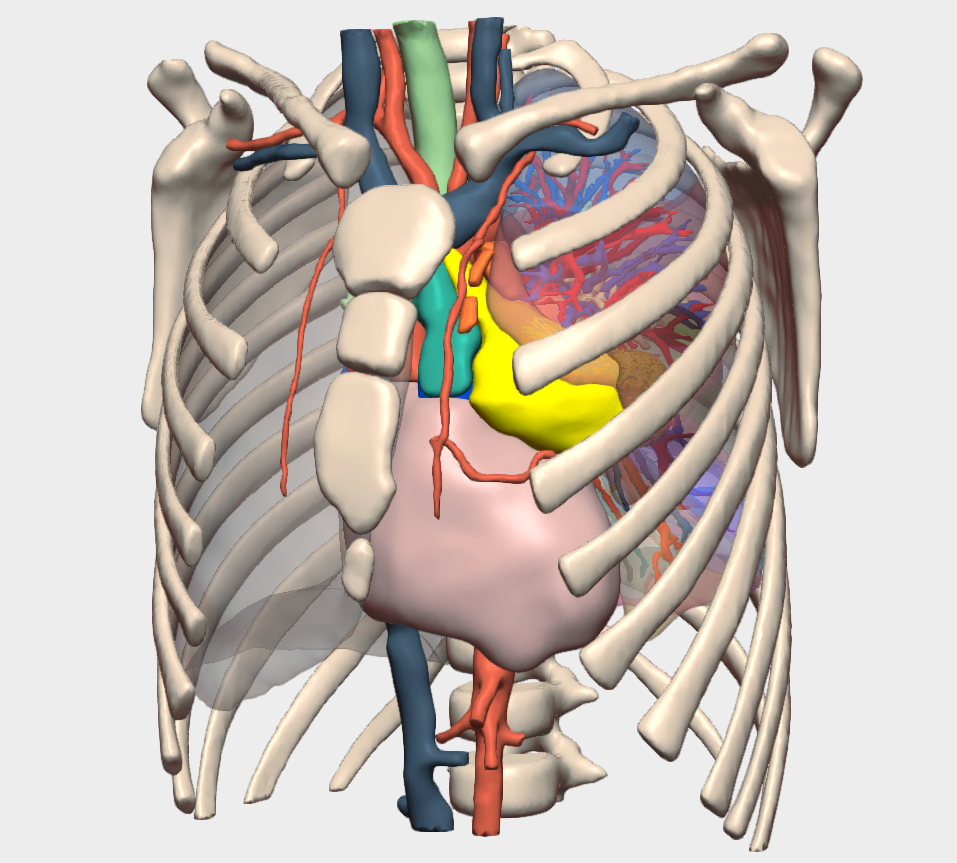
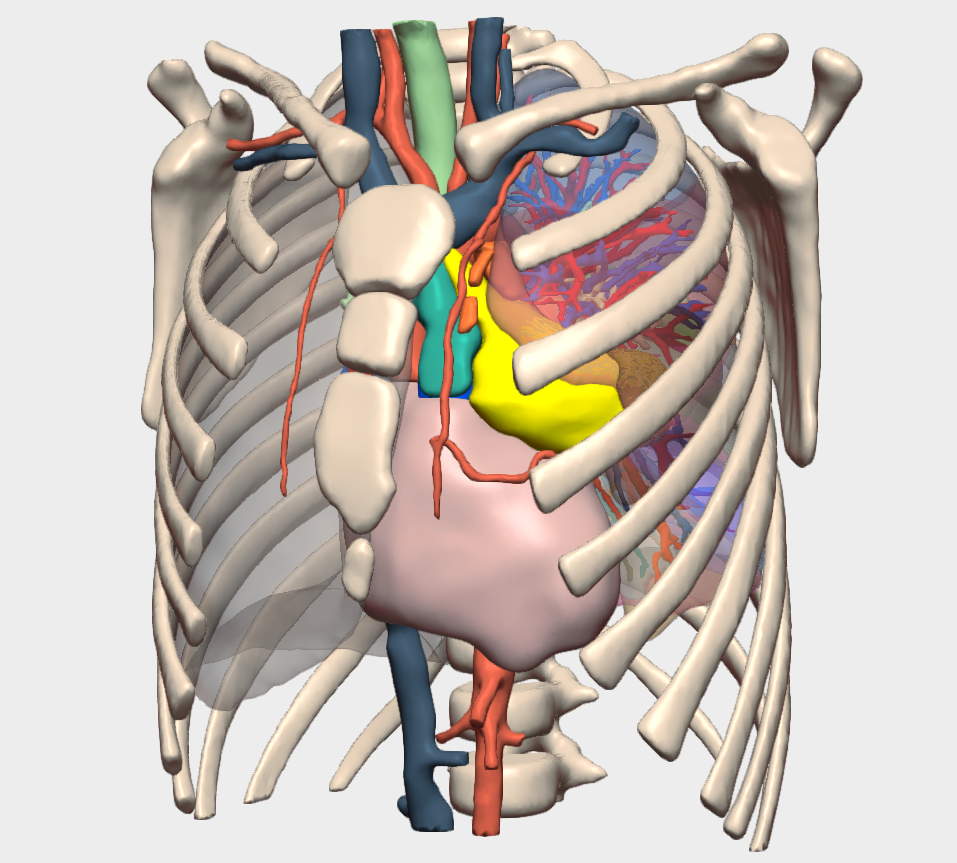
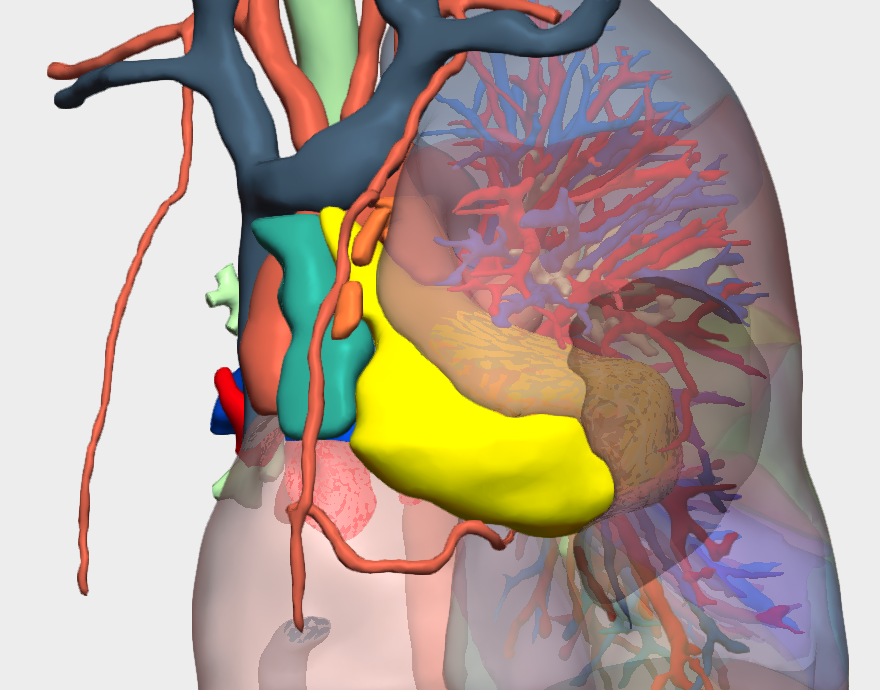
Costal Ewing sarcoma is a malignant tumour arising from bone or adjacent soft tissues of the thoracic cage, most commonly affecting children and young adults. Due to its aggressive behaviour and complex anatomical location, surgical treatment is particularly challenging. Preoperative planning supported by patient-specific 3D models allows highly accurate visualisation of tumour extent and its relationship with critical structures such as the lungs, heart and spine. This approach enhances surgical safety, supports a more precise operative strategy and contributes to improved oncological and functional outcomes.
Clinical Case Presentation
We report the case of an 8-year-old paediatric patient diagnosed with a left-sided costal Ewing sarcoma. Imaging studies revealed that the tumour was adherent to the pericardium and parietal pleura, presenting a technically demanding surgical scenario.
Surgical Management of Ewing Sarcoma
The procedure was performed by Dr Carmen Benlloch, Paediatric Surgeon at Hospital Clínico Universitario de Valencia. The surgical approach included:
-
Complete resection and disarticulation of the second rib, where lytic changes had been identified on imaging, together with the associated intercostal musculature.
-
Partial resection of the first and third ribs.
-
En bloc excision of the tumour, extending from the second to the sixth rib along the anterior axillary line.
-
Careful release of tumour adhesions to the pericardium, which was confirmed to be free of tumour infiltration on histopathological examination.
-
Resection of the involved chest wall with partial excision of the parietal pleura.
-
Reconstruction using a Lactosorb plate on the first rib and a Gore-Tex patch to repair the chest wall defect.
Preoperative imaging had suggested a smaller tumour size and possible pericardial infiltration. However, intraoperative findings confirmed the absence of pericardial invasion.
3D Surgical Planning and Outcomes
The use of a patient-specific 3D model was critical in the preoperative planning phase. It enabled the surgical team to accurately confirm that the tumour extended from the second to the sixth rib and was in contact with, but did not infiltrate, the pericardium—findings that were fully corroborated during surgery.
Thanks to this advanced 3D planning, a radical tumour resection was achieved while minimising morbidity, ensuring the best possible outcome for the patient.
¡Follow us on social media to stay up to date with our latest updates!