Pleural mesenchymal tumours are rare neoplasms that most commonly originate from the parietal pleura. In certain cases, these tumours may reach considerable size, occupying a large portion of the hemithorax and displacing critical structures such as the lungs and the thoracic cavity.
The use of 3D models in thoracic surgery enables detailed visualisation of the relationship between the tumour and adjacent anatomical structures, supports optimal surgical strategy selection, and helps prevent injury to vital organs and vessels.
Clinical Case Description
This case involves a 55-year-old female patient, a former smoker, with no history of thoracic surgery, who was under follow-up for a large pleuropulmonary mass in the left hemithorax. Histopathological analysis of an ultrasound-guided biopsy confirmed the diagnosis of an intermediate-risk mesenchymal tumour, according to the Demicco classification.
Imaging studies revealed a mass measuring 150 × 130 × 90 mm, with close anatomical relationship to the diaphragm, extensive contact with the parietal pleura, and compression of the underlying lung parenchyma. The most relevant features of the lesion included marked hypervascularisation and the presence of aberrant vascular supply, with arterial inflow from the coeliac trunk and venous drainage into the inferior pulmonary veins. These characteristics significantly increased the risk of intraoperative haemorrhage.

In addition, the patient presented with mild left ventricular systolic dysfunction (LVEF 45–50%) in the context of left bundle branch block (LBBB), as well as moderate restrictive ventilatory impairment on pulmonary function testing (FVC: 67%, FEV₁: 52%, DLCO: 82%).
The main challenges identified were:
- Extrapulmonary origin and complex tumour vascular pedicle, with a high risk of bleeding
- Extensive anatomical relationships with the pleura, diaphragm and mediastinal structures
- The need to preserve as much functional lung tissue as possible, given the patient’s limited respiratory reserve
Value of the 3D Model in Surgical Planning
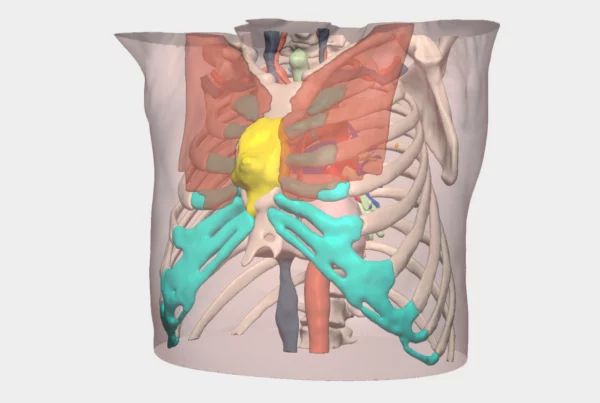
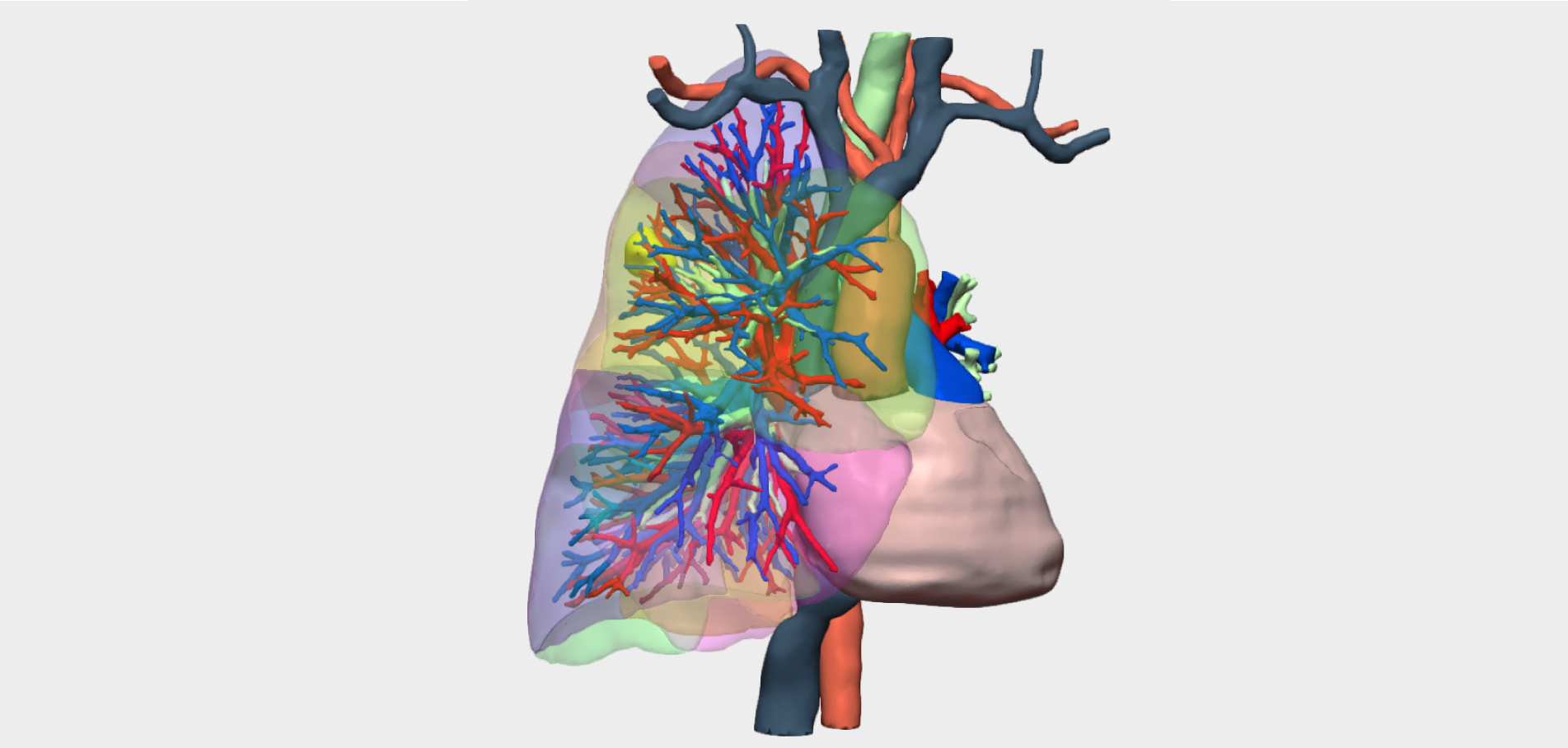
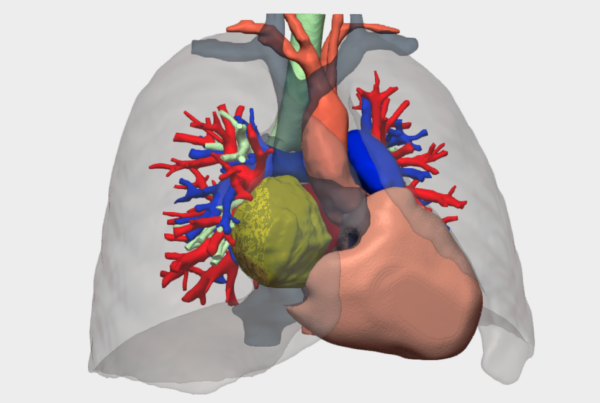
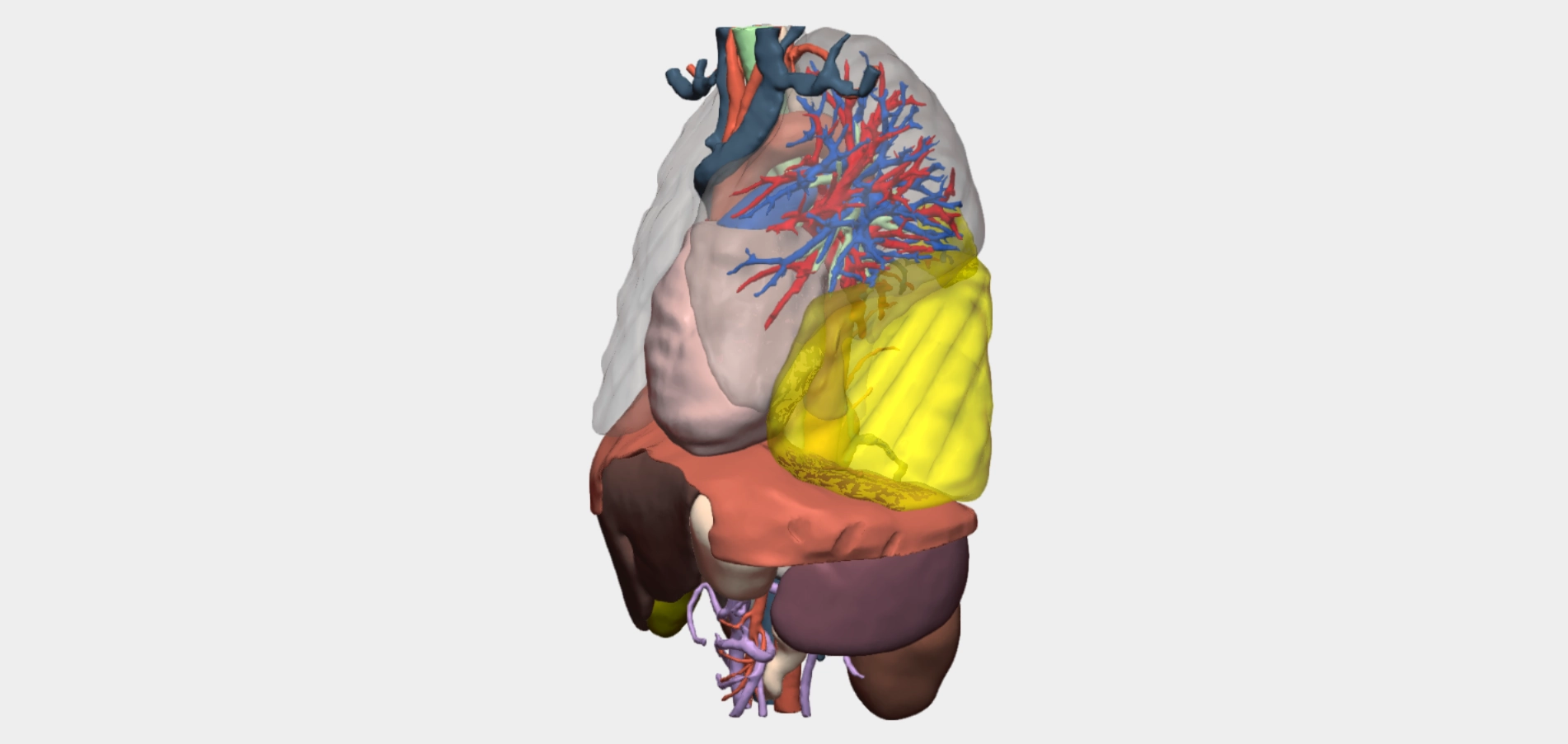
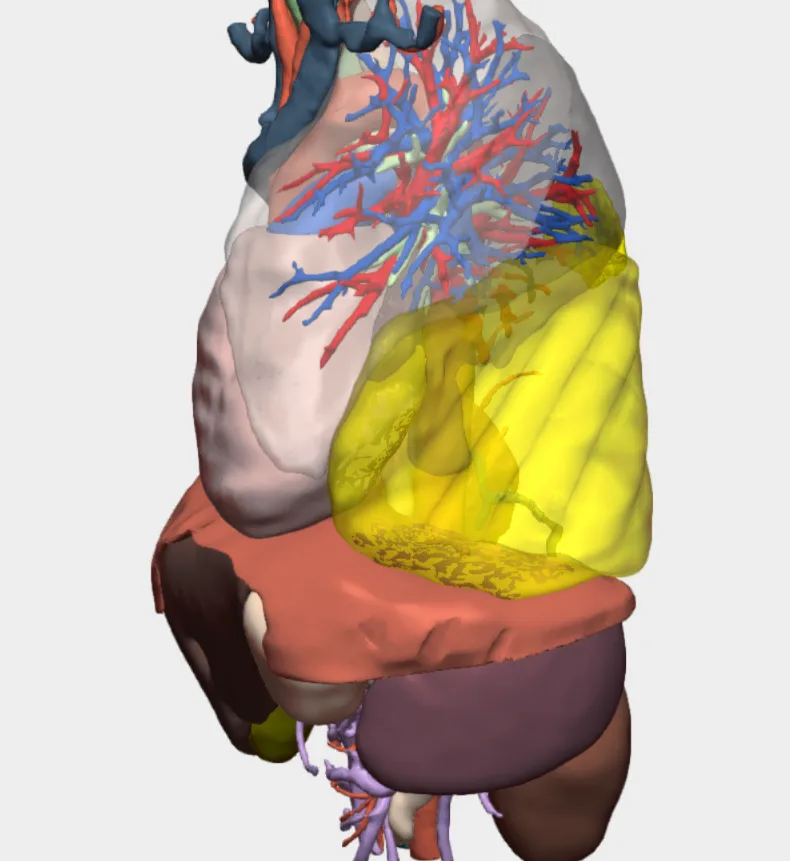
Given the anatomical and functional complexity of the case, a high-resolution 3D reconstruction based on contrast-enhanced CT imaging was requested from Cella Medical Solutions. The specific objective was to achieve detailed identification of the arterial and venous supply of the giant pleural fibrous tumour in the left hemithorax. Based on conventional imaging, arterial supply from the coeliac trunk and venous drainage into the pulmonary venous system were suspected.
The 3D model provided decisive value during the preoperative phase:
- Confirmation of the aberrant vascular pathways, enabling precise visualisation of arterial branches arising from the coeliac trunk and their course towards the tumour at the thoracic base
- Identification of venous drainage into the inferior pulmonary veins, which was critical for safe intraoperative vascular control
- Volumetric and spatial assessment of the tumour’s relationship with adjacent structures, including the diaphragm, pulmonary hilum, posterior mediastinum and surrounding lung parenchyma
- Use of advanced digital 3D tools such as virtual cutting planes, rotation and interactive manipulation, together with physical 3D printing for surgical simulation and multidisciplinary discussion
- Improved coordination with Interventional Radiology, allowing optimal planning of selective arterial embolisation 48 hours prior to surgery
Thanks to the 3D reconstruction, additional preoperative angiographic studies were deemed unnecessary, streamlining decision-making and optimising clinical timelines.
Angiography and Embolisation Report
The patient underwent selective arteriography 48 hours prior to surgery. The procedure confirmed tumour arterial supply from aberrant branches of the coeliac trunk, particularly hypertrophied left ascending diaphragmatic and lower intercostal arteries.
elective embolisation of the tumour-feeding arteries was performed using calibrated particles and microcoils, achieving effective vascular occlusion without immediate complications. Post-embolisation angiographic control demonstrated absence of significant arterial flow to the tumour mass.
This step was crucial in reducing intraoperative bleeding risk and facilitating safer surgical dissection.
Surgical Outcome
Surgery was performed via left lateral thoracotomy, with en bloc resection of the tumour. A non-anatomical segmentectomy of the basal segment of the left lower lobe was carried out, preserving the remaining lung parenchyma.
Thanks to preoperative arterial embolisation and precise planning supported by the 3D model, the procedure was completed without intraoperative complications, with effective vascular control and no need to extend the planned resection. The patient showed favourable postoperative evolution and was discharged without complications.
Conclusions
3D model-assisted surgical planning, combined with selective arterial embolisation guided by arteriography, was decisive in the success of this complex intervention. Three-dimensional visualisation allowed anticipation of technical challenges, optimisation of the surgical strategy, and mitigation of risks associated with high tumour vascularity.
This case highlights the clinical value of integrating advanced technologies such as 3D reconstruction into complex thoracic surgery, particularly in the management of vascular pleural tumours, and underscores the importance of close multidisciplinary collaboration between surgery, interventional radiology and preoperative planning teams.
Follow us on social media to stay up to date with our latest clinical cases and technological innovations.