
“3D reconstruction using the Cella system enabled a detailed and comprehensive understanding of the anatomical relationships of the lesions to be resected, reducing the risk of iatrogenic injury, anticipating critical steps and key surgical maneuvers, and enhancing overall procedural safety for both the surgical team and the patient.”

Dr. Felipe Sáez – Consultant Urologist at the Urology Unit, Virgen de la Victoria University Hospital, Málaga
Clinical Case
A 19-year-old male, referred from another center, with a history of right radical orchiectomy for a testicular mass. Histopathological analysis revealed a mixed germ cell tumor, composed of 70% yolk sac tumor and 30% postpubertal teratoma, with lymphovascular invasion. The disease was staged as pT2 N3 M1, with findings including a retroperitoneal nodal conglomerate, left para-aortic retroperitoneal lymphadenopathy suggestive of metastasis, and left paravertebral, intrathoracic, and extrapulmonary nodules.
- Given the clinical stage, the case was evaluated by Medical Oncology, which initiated four cycles of Bleomycin, Etoposide, and Cisplatin (BEP). Baseline tumor markers were LDH 350 (1.42 × ULN), β-hCG <1, and AFP 961.
- After the first cycle, the patient developed deep vein thrombosis (DVT) and pulmonary embolism (PE), requiring initiation of anticoagulation with low-molecular-weight heparin (10,000 IU daily).
- The patient completed the four cycles of BEP, with post-treatment tumor markers of β-hCG <1 and AFP 2.8.
On re-evaluation with CT imaging after completion of chemotherapy, there was persistence of multiple necrotic-appearing left paravertebral and paracostal masses, which showed progression compared to the previous study.
Increase in size of the retroperitoneal nodal conglomerate, which encases and mildly compresses the aorta and collapses the inferior vena cava, with vascular infiltration not excluded.
The distal common iliac, external iliac, and right internal iliac veins are completely filled with hypodense material, consistent with deep vein thrombosis.
Grade II/IV right ureteropelvicalyceal dilatation secondary to obstruction of the proximal right ureter at the level of the nodal conglomerate.
In view of these findings, the patient was referred to our center for evaluation for retroperitoneal lymph node dissection (RPLND) due to persistent post-chemotherapy retroperitoneal masses.
3D Planning and Tools
A Cella 3D study was requested due to:
- The distribution of the retroperitoneal masses to be surgically addressed
- Their relationship with the aorta and inferior vena cava
- Right ureteral involvement as well as collapse of the inferior vena cava
- The need for improved characterization of the lesions and their relationships with adjacent anatomical structures, in order to reduce the risk of injury to these structures during surgery.
Adopted Surgical Strategy
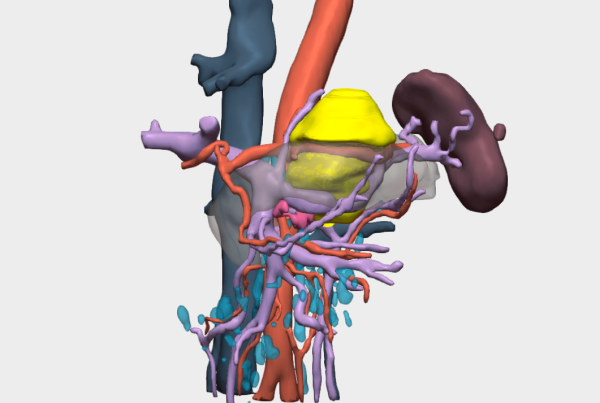
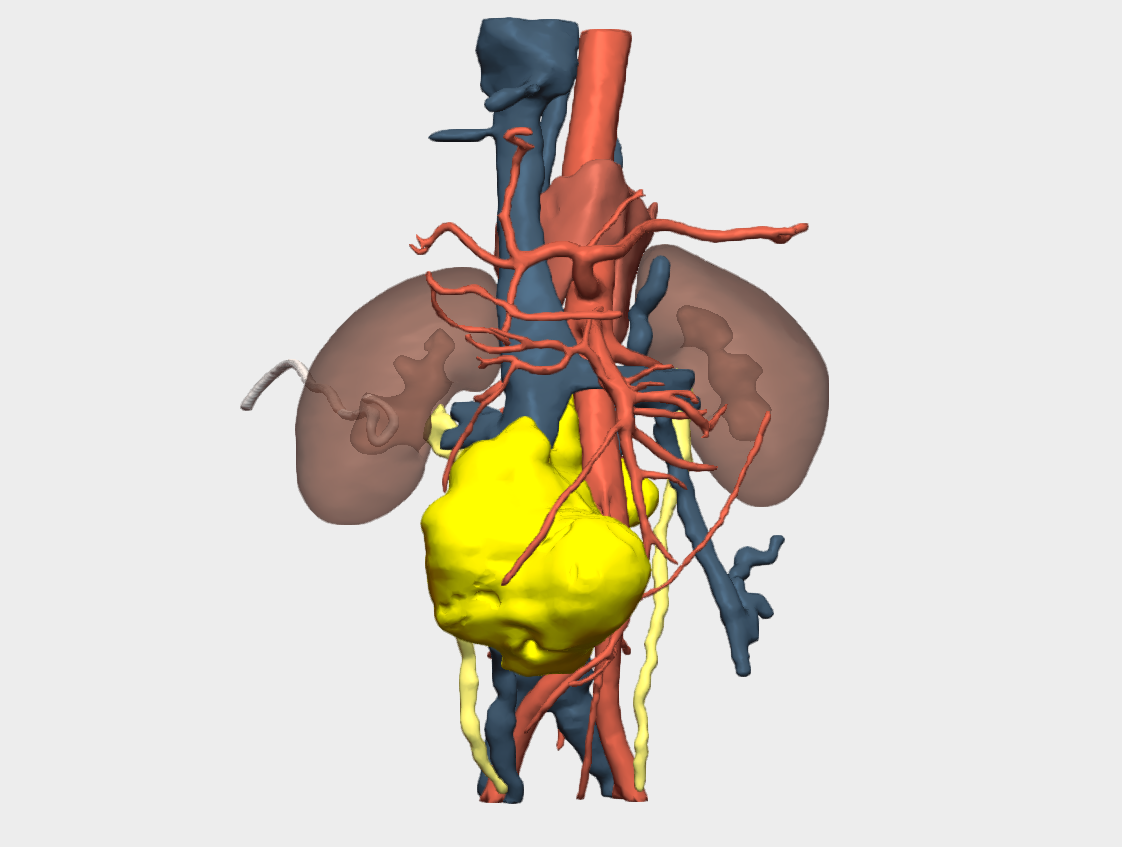
Prior to surgery, urgent placement of a right percutaneous nephrostomy was requested to preserve right renal unit function, given the entrapment caused by the retroperitoneal mass as demonstrated on CT and on the 3D reconstruction (Figure 1).
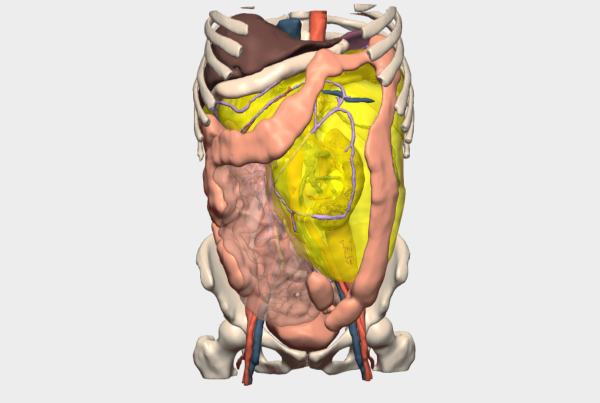
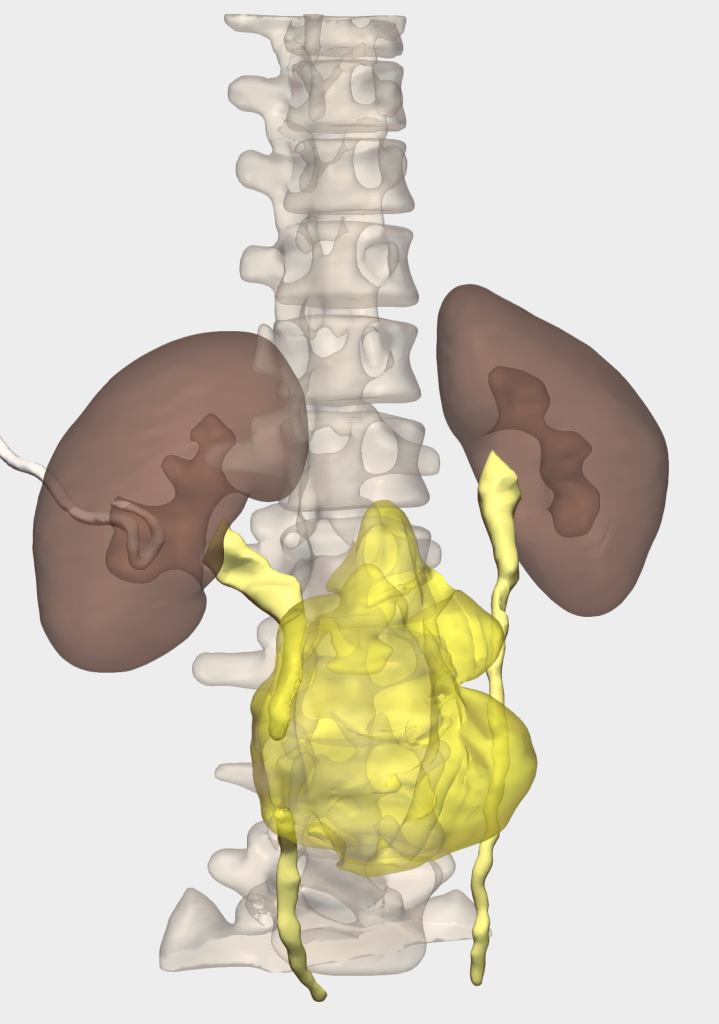
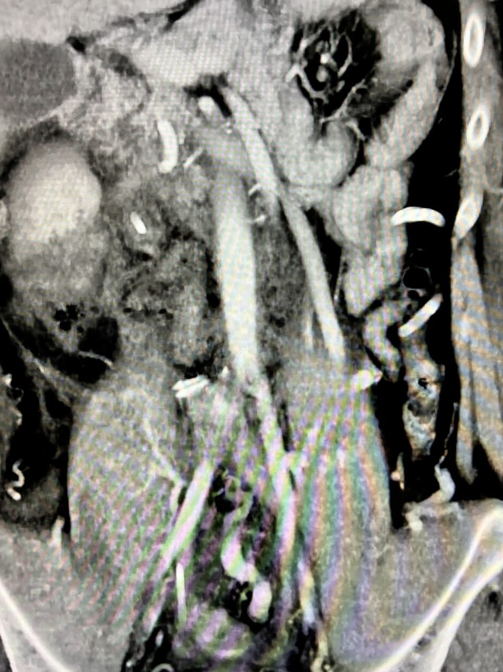
A CT angiography (CTA) was also requested to assess vascular relationships and enable three-dimensional reconstruction using the Cella system. Additionally, an inferior vena cava (IVC) filter was placed via right jugular vein access at the L1 level (left juxtarenal position), as there was no available space below the renal vasculature. This was performed to allow safe discontinuation of anticoagulation prior to surgery (Figure 2).

3D Models Tools
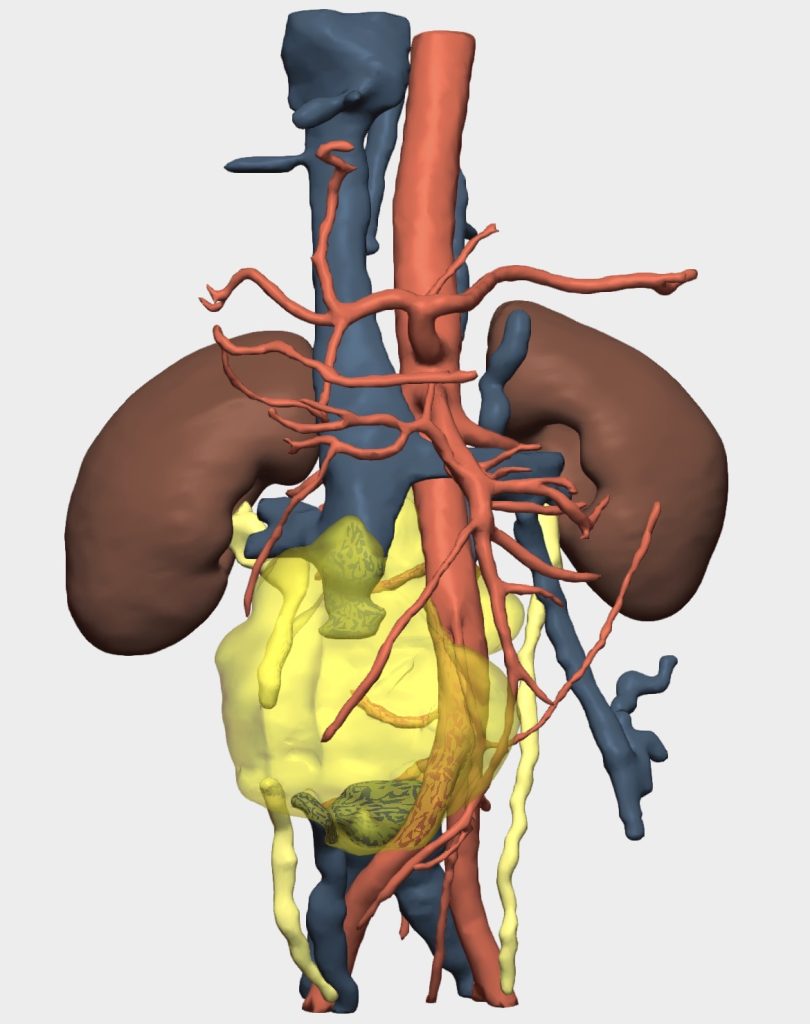
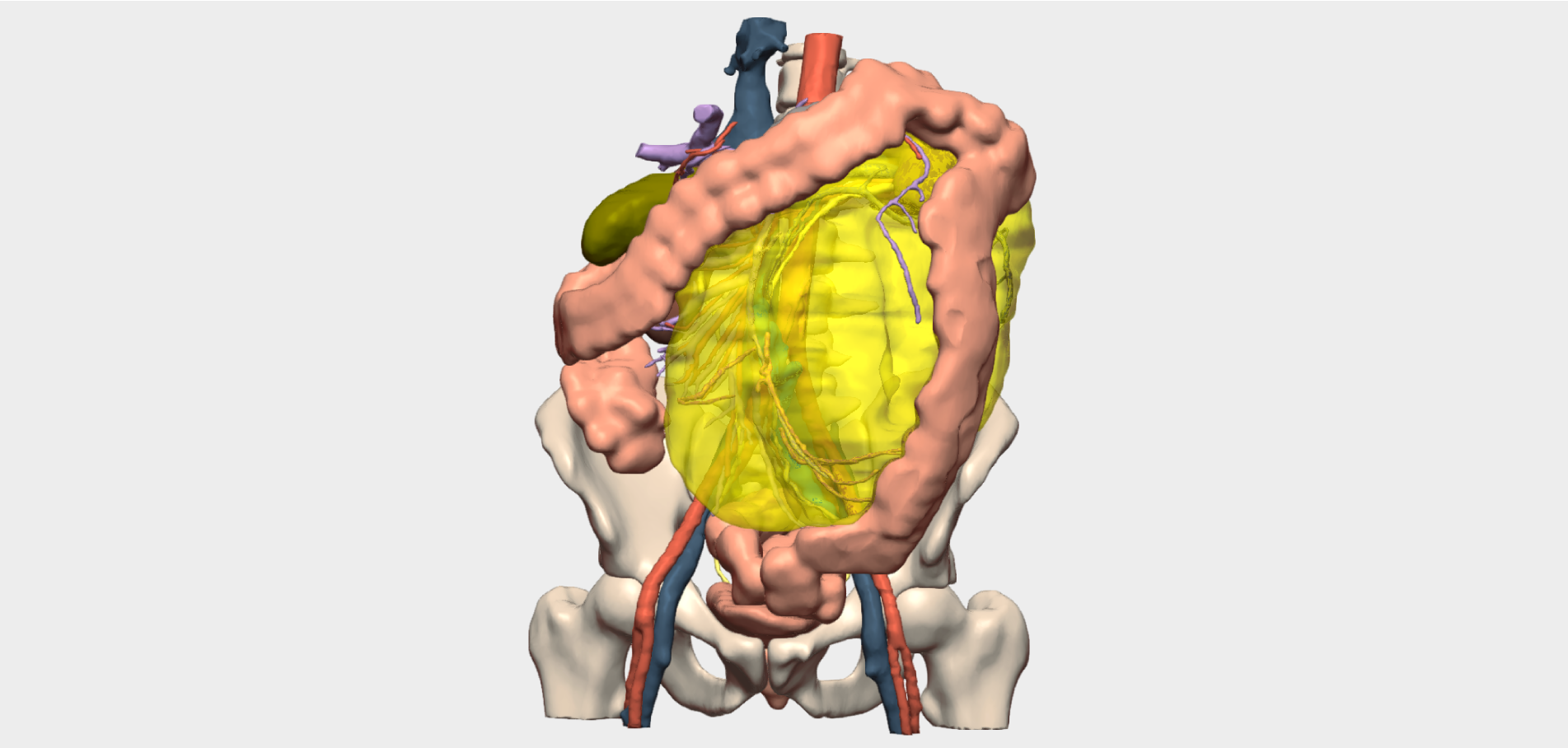
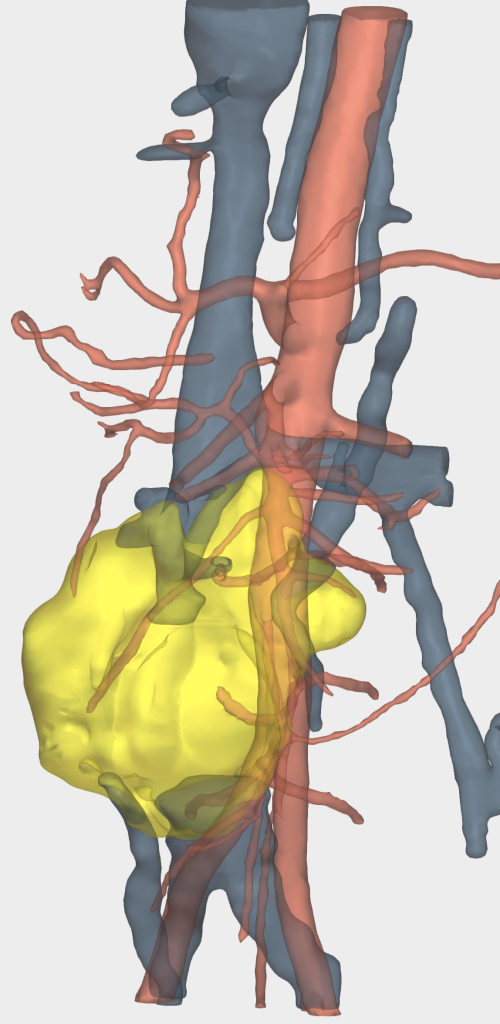
The 3D reconstruction enabled:
- Assessment of the anatomical spaces and relationships of the masses
- Identification of the lumbar arteries and veins in close contact with the lesions
- Evaluation of the azygos and hemiazygos systems in terms of patency in the context of inferior vena cava collapse, as well as the relationship between the right ureter and the masses (Figure 3)
Surgical Procedure
A midline xiphopubic laparotomy was performed, providing access to the abdominal cavity. The ascending colon and small bowel were fully mobilized up to the ligament of Treitz, allowing entry into the retroperitoneal space.
- Fibrotic and necrotic nodal conglomerates, as previously described, were identified. Careful dissection and mobilization were performed, beginning with the precaval and preaortic regions, with preservation and visualization of both intact common iliac vessels, as well as the inferior mesenteric artery.
- Due to dense adherence to the right ureter, en bloc resection of the involved ureteral segment together with the nodal conglomerate was performed.
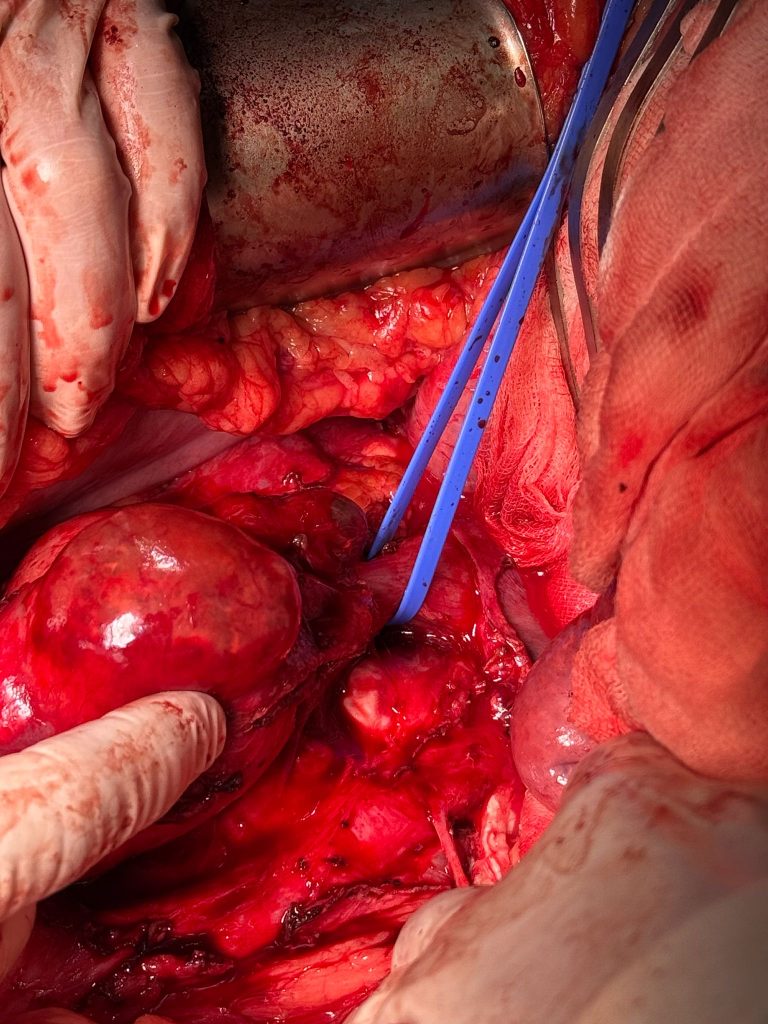
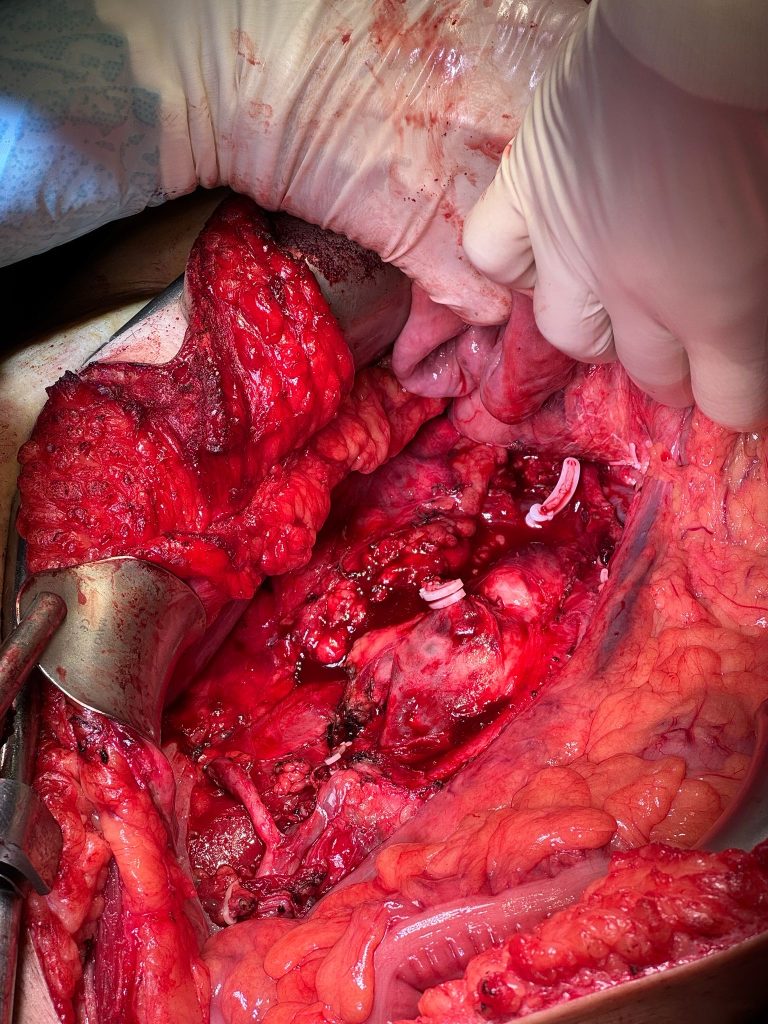
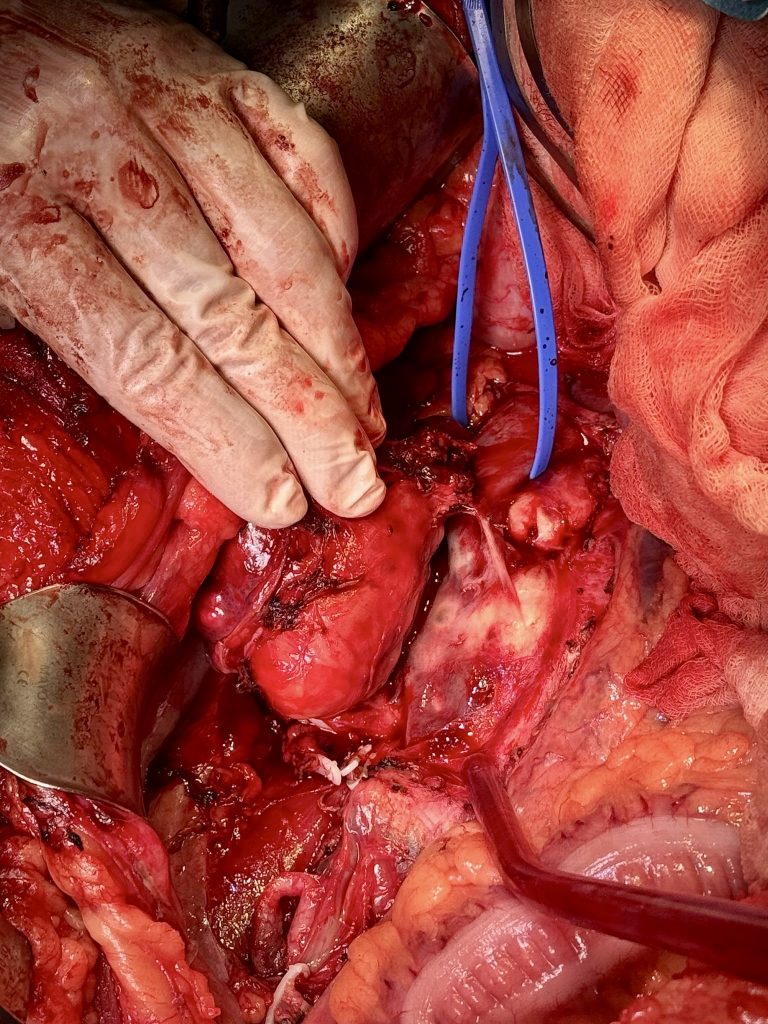
- Similarly, the inferior vena cava (IVC) was found to be densely adherent. It was dissected both cranially and caudally, and after vascular control with a vessel loop, clamping of the IVC produced no hemodynamic instability, confirming adequate collateral circulation.
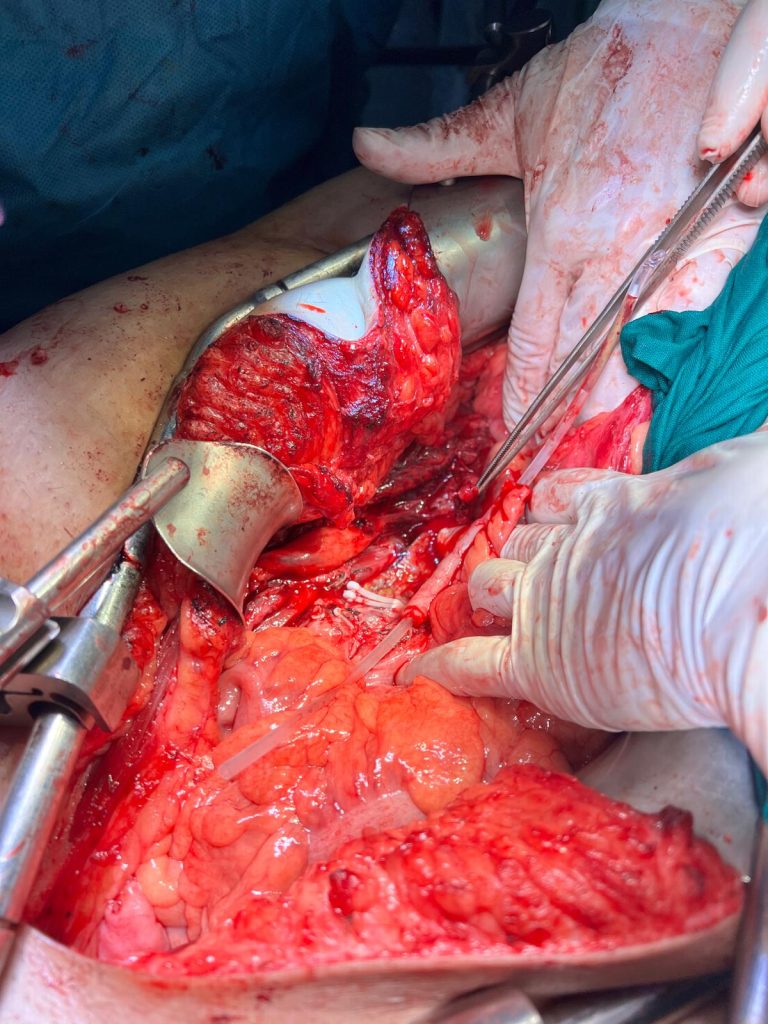
- A cavectomy was therefore carried out, with placement of three Hem-o-lok clips proximally and distally to the conglomerate, followed by division using scissors (Figures 4, 5, and 6).
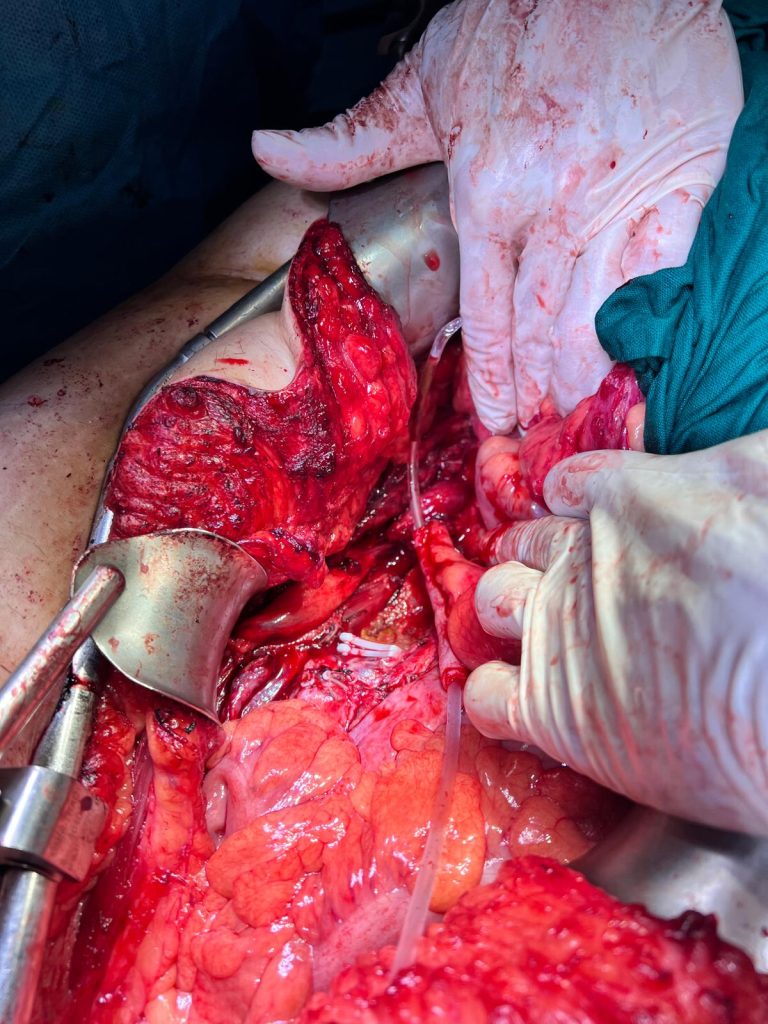
- Dissection of the remaining lymphadenopathy was performed (Figures 7 and 8).
- Lymphatic leakage was controlled using clips and Hem-o-lok devices.
- The lower pole renal attachments were released. Proximal and distal ureteral dissection confirmed that end-to-end anastomosis was not feasible; therefore, ureteral substitution using the cecal appendix was performed (Figures 9 and 10).
- A nephropexy to the psoas muscle was carried out using V-Loc 3/0 suture.
- The appendix was transected at the cecal level using LigaSure, preserving the mesoappendix.
- The appendix was opened and spatulated, as was the ureter.
- Uretero-appendiceal anastomosis was performed using a continuous 3/0 Monocryl suture. A 4.8 Fr double-J ureteral stent was placed under guidance.
- An omental flap was used to cover the ureteroplasty. Closure was performed with V-Loc suture.

The patient subsequently had an uneventful postoperative course and was discharged on postoperative day 12, following a CT scan performed to rule out collections or complications (Figure 11).
The inferior vena cava filter was removed 21 days after surgery without complications. The double-J stent and right nephrostomy were removed 40 days postoperatively, following a CT urography that ruled out contrast leakage.
Histopathological analysis revealed postpubertal teratoma and yolk sac tumor. The patient is currently undergoing a new line of chemotherapy due to the presence of viable tumor.
Surgery performed by Dr. Cantero, Dr. Amores, Dr. Sáez, and Dr. Herrera (in order of appearance), from the Department of Urology at Virgen de la Victoria University Hospital, Málaga.

Follow us on social media to stay up to date with our latest updates!