“3D planning was key to identifying vascular involvement that was not clearly visible on conventional imaging, which radically changed the surgical strategy: from an initially planned hepatic resection to liver transplantation after neoadjuvant therapy, thereby avoiding a non-oncologic surgery”.

Dra. Eva María Montalvá Orón, Specialist in General and Digestive Surgery at Hospital Universitario y Politécnico La Fe.
Caso Clínico
57-year-old female patient diagnosed with suspected hilar cholangiocarcinoma (January 2025) after admission for abdominal pain associated with elevated cholestatic enzymes, mildly increased bilirubin levels, and generalized pruritus.
Radiological studies performed at the referring center (MRCP and thoracoabdominal CT scan) revealed a 15 mm stenosing lesion located at the hilar confluence, showing contrast enhancement and suggestive of intraductal perihilar cholangiocarcinoma.
The case was presented at the Hepatobiliary–Pancreatic (HBP) tumor board, where a left hepatectomy initially appeared feasible, as imaging showed continuity between the right anterior and posterior sectoral ducts with a common right duct stump.
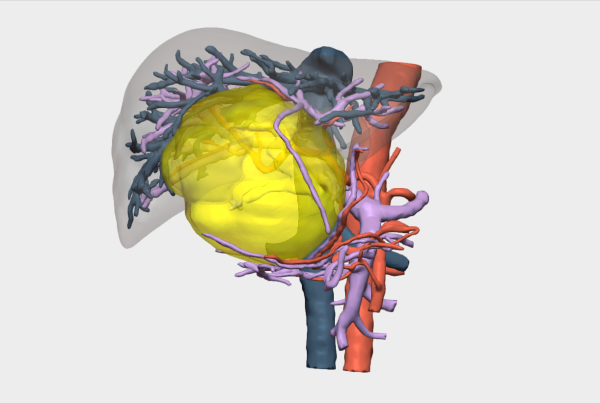
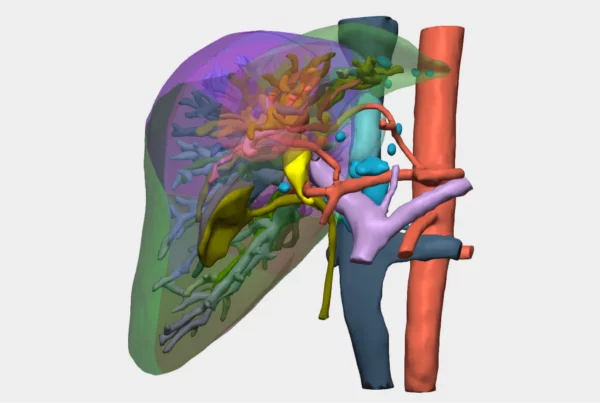
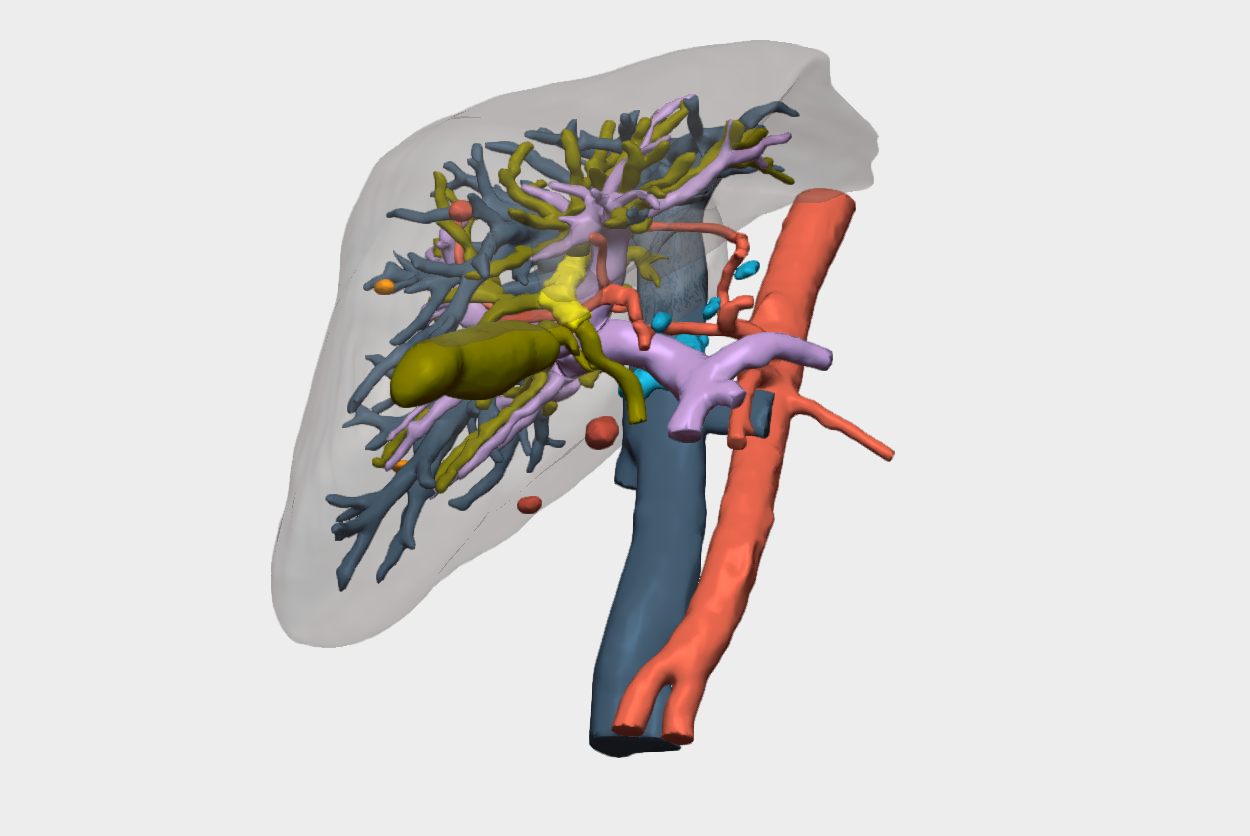
Relevant findings on 3D reconstruction
- Involvement of the biliary confluence extending to the right ductal radicals.
- Involvement of the right hepatic artery (encased within the lesion) → rules out left hepatectomy.
- Left portal vein encompassed by the lesion, with a small distal margin in the left portal vein, insufficient to perform a venous anastomosis.
- High complexity for right trisectionectomy with portal confluence resection.
Given this scenario, and after excluding hilar lymphadenopathy and extrahepatic disease through imaging studies and endoscopic ultrasound, the decision was made to proceed with neoadjuvant therapy and consider liver transplantation as the preferred therapeutic option.
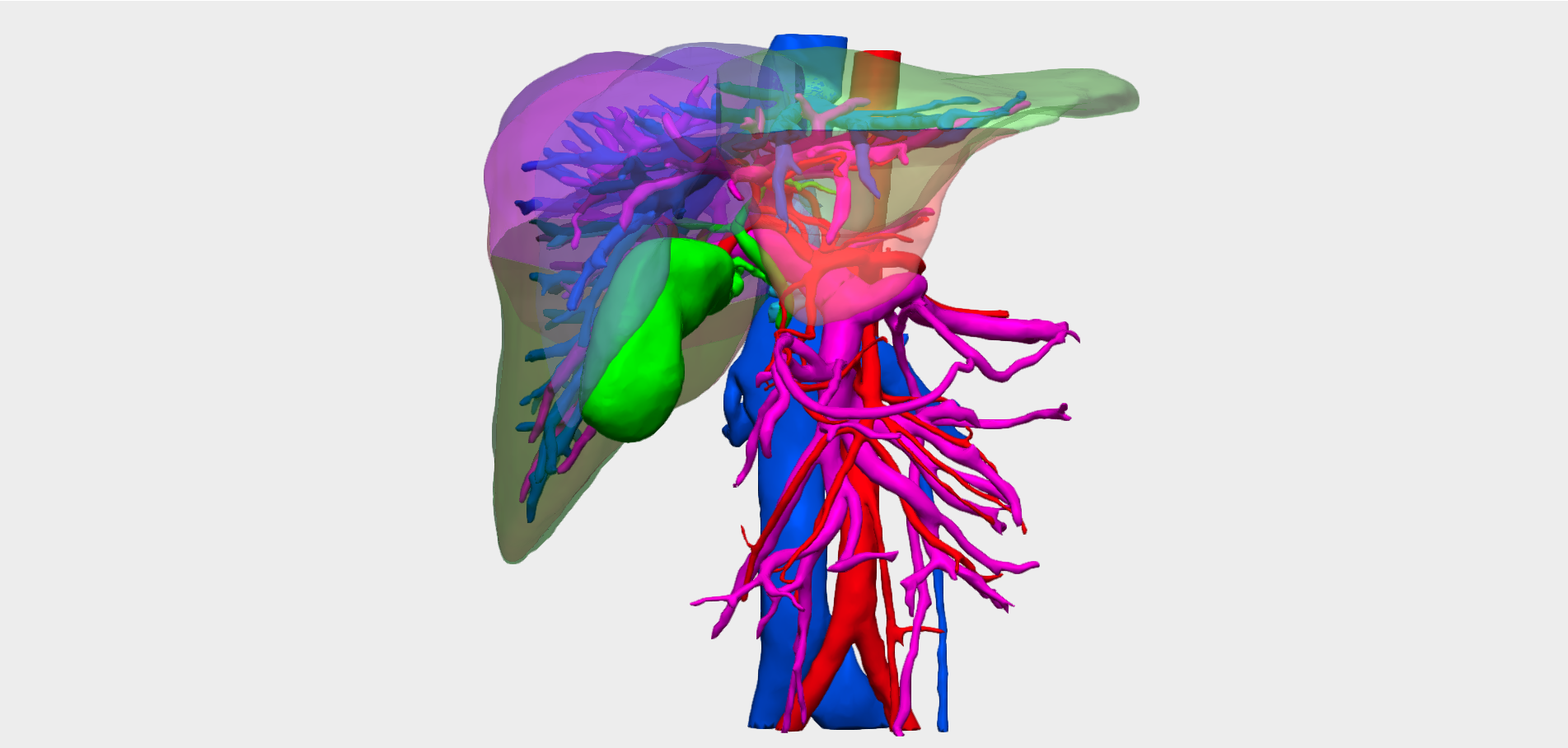
3D Planning
In this case, a more accurate definition of the extent of the disease allowed us to rule out hepatic resection (which can be technically demanding in this setting) and to refer the patient for liver transplantation following neoadjuvant therapy (cisplatin–gemcitabine chemotherapy and radiotherapy), a novel indication in the treatment of this pathology.
Surgical Strategy and Outcomes
Following completion of neoadjuvant therapy and confirmation of no disease progression or extrahepatic spread, the patient was referred for liver transplantation evaluation.
During surgery, extrahepatic involvement was ruled out by intraoperative pathological assessment, including analysis of the distal bile duct resection margin. Liver transplantation was then performed, with interposition of an arterial graft between the aorta and the hepatic artery of the liver graft.
An extensive lymphadenectomy was carried out, and the portal vein was transected as far as possible from the bifurcation. Due to the absence of portal hypertension, collateral circulation, or underlying liver parenchymal disease, a venous graft was required to establish a temporary porto-caval shunt during the procedure.
Key Aspects in Surgical Planning
- Tumor location in relation to the biliary tree and the arterial and portal vessels was decisive.
- Virtual navigation proved essential in assessing potential vascular infiltration.
- On conventional imaging studies, it can be difficult to distinguish between mere tumor contact and true vascular invasion.
- Establishing unresectability prior to surgery is crucial in order to:
- Reduce morbidity and mortality.
- Avoid non-curative oncologic surgeries.
- Enable a strategic shift in the surgical approach when necessary.
Liver transplantation was performed, achieving complete oncologic eradication of the disease.
The surgery was carried out by Dr. Eva Montalvá Orón (Hepatobiliary–Pancreatic Surgery and Transplant Unit, Hospital Universitario y Politécnico La Fe) and Dr. David Calatayud Mizrahi (Hepatobiliary–Pancreatic Surgery and Transplant Unit, Hospital Universitario y Politécnico La Fe).
Follow us on social media to stay up to date with our latest updates!