
“The 3D model provided a high level of confidence during surgical planning, particularly in assessing the tumour’s relationship with adjacent anatomical structures and the extent of infiltration. This enabled complete tumour resection without complications”

Dra. Raquel Alfonso, General and Digestive Surgeon, Hospital Clínico Universitario de Valencia
Clinical Case Presentation: Large Adrenocortical Carcinoma
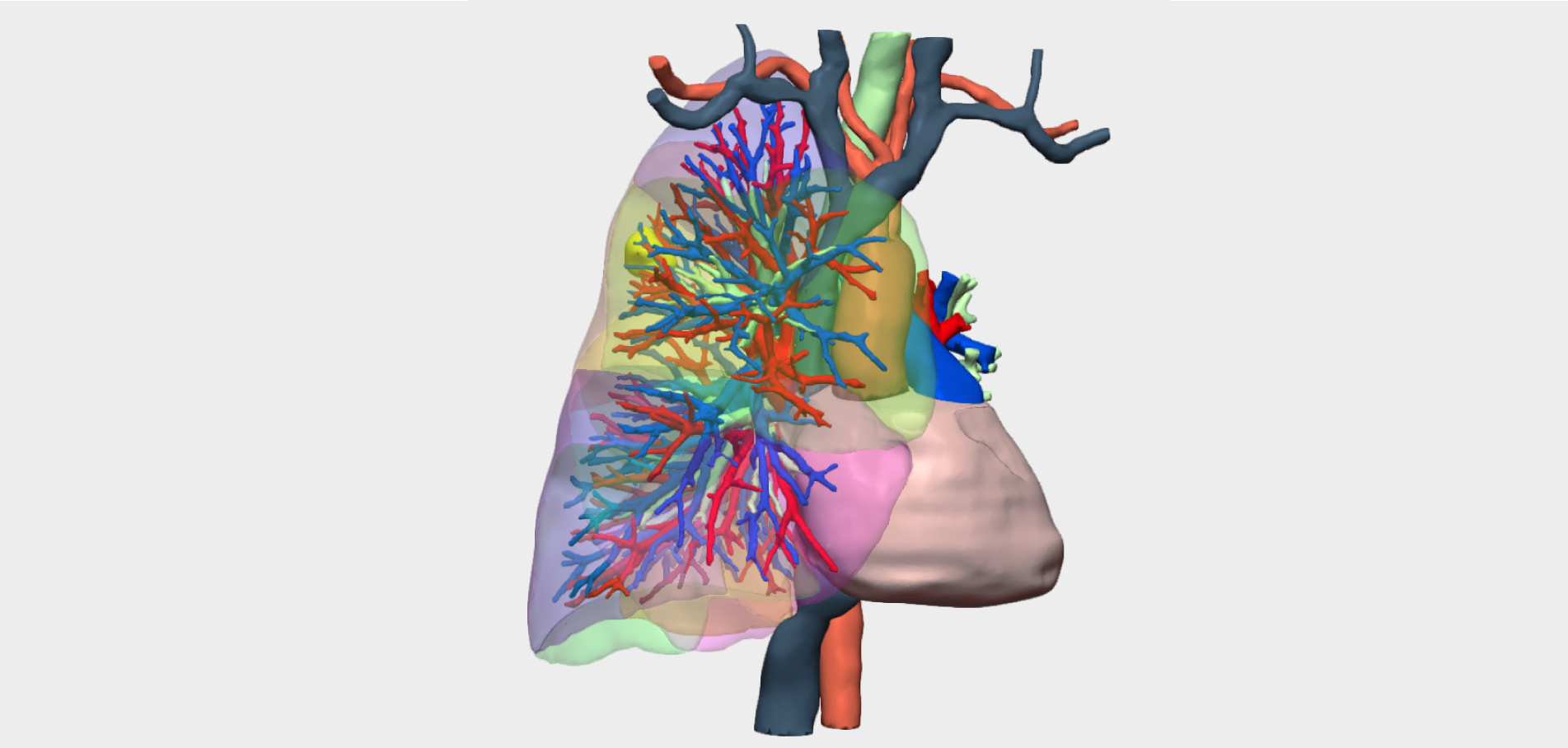
This case describes a 45-year-old male patient with no relevant medical history, who presented with lower back pain. Diagnostic imaging studies, including abdominal ultrasound and CT scan, revealed a large right adrenal mass measuring 25 × 30 cm, consistent with adrenocortical carcinoma, associated with bilateral pulmonary metastases.
The adrenal tumour did not secrete catecholamines; however, it produced sex hormones and cortisol. Following multidisciplinary discussion within the Endocrine Tumour Board, surgical resection of the adrenocortical carcinoma was proposed with the aim of reducing tumour burden and facilitating subsequent adjuvant therapy.
Radiological Findings and Surgical Complexity
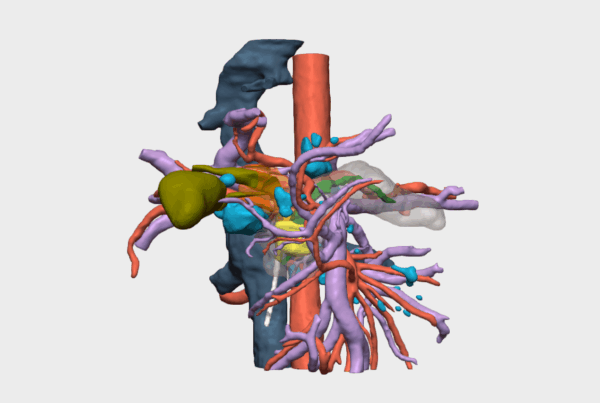
Abdominal CT imaging demonstrated a complex mass with the following characteristics:
- Inferior displacement of the right kidney
- Extensive collateral vascular circulation
- Significant compression of the Inferior Vena Cava (IVC) at the juxtahepatic level, raising concerns regarding potential vascular infiltration
- Suspected involvement of the hepatic surface
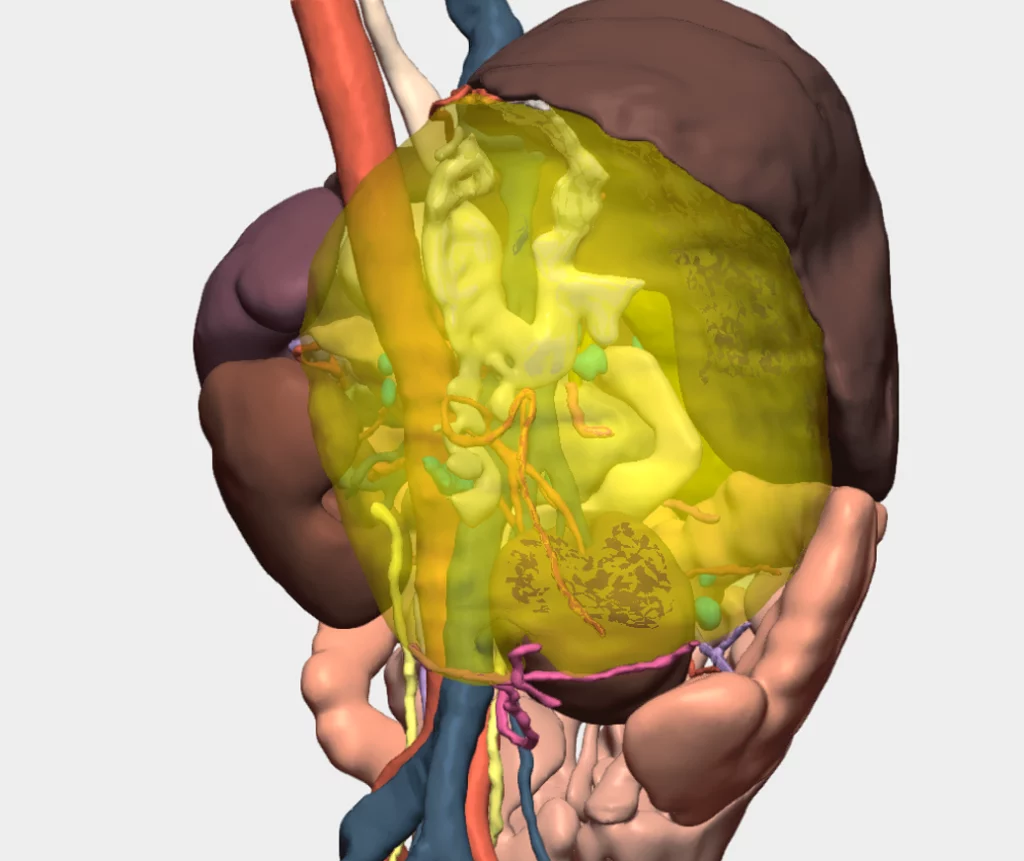
These findings indicated a high level of surgical complexity, primarily due to the tumour’s close proximity to critical vascular structures.
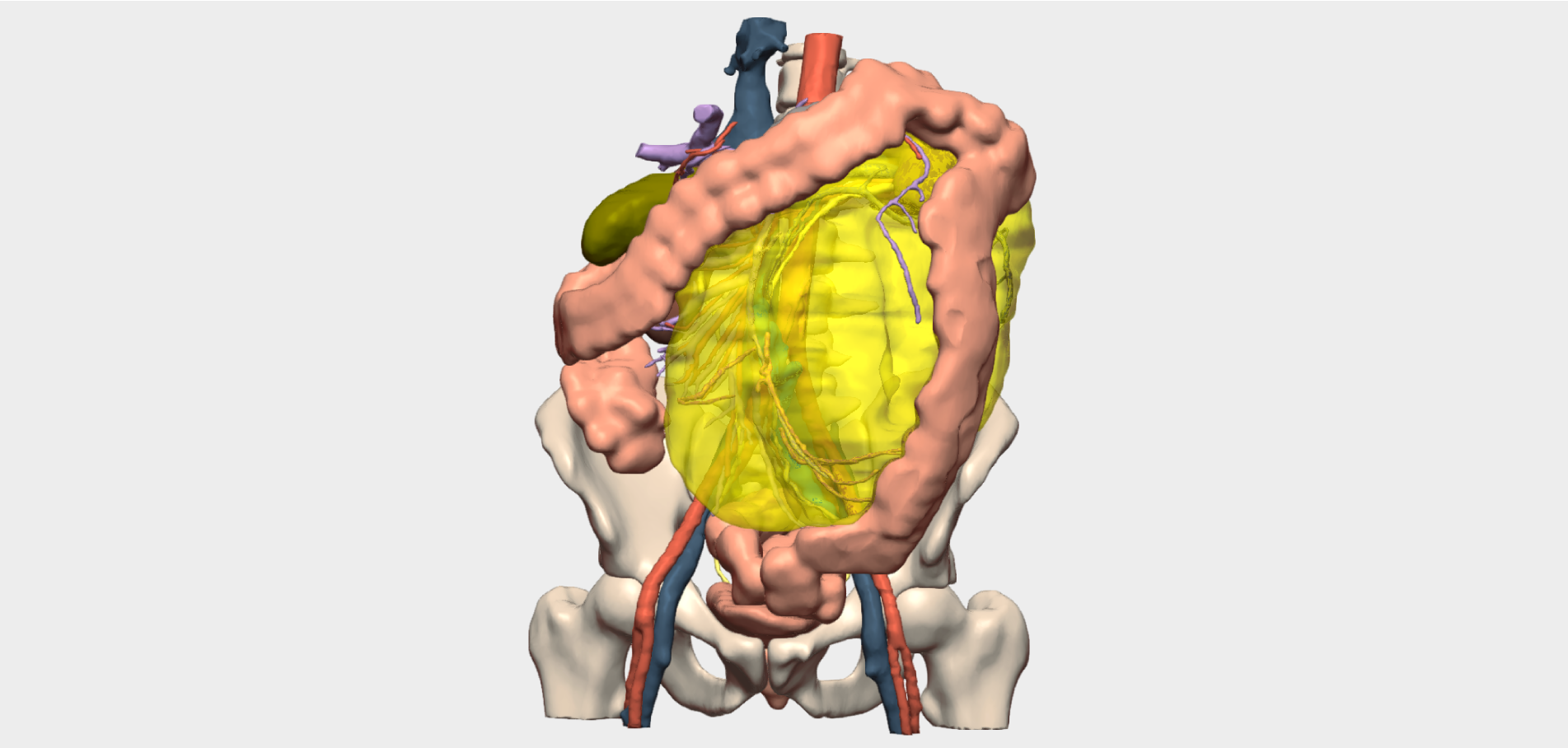
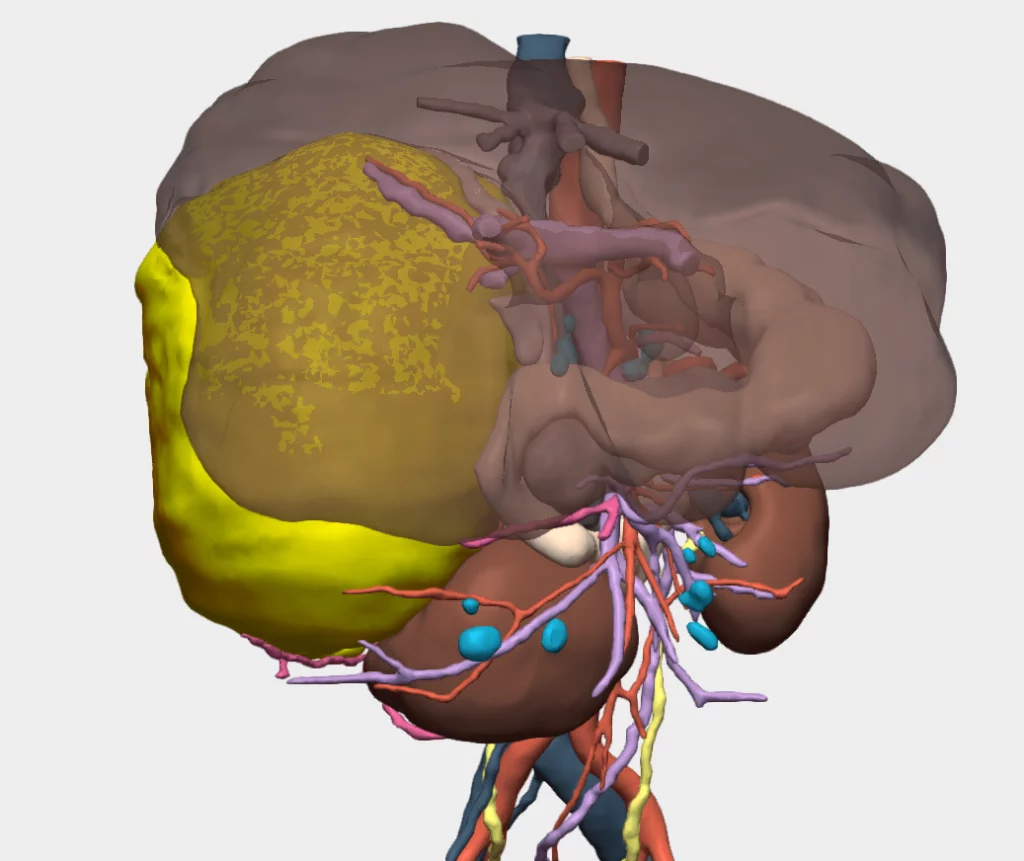
Surgical Planning with a 3D Model: Innovation in the Management of Adrenocortical Carcinoma
To complement diagnostic imaging and accurately assess the anatomical relationships of the adrenal tumour, a patient-specific 3D model was requested. The primary objective was to precisely evaluate the point of contact with the Inferior Vena Cava and to confirm or exclude vascular infiltration.
Based on the insights provided by the 3D model, surgical resection was planned and performed by the Endocrine Surgery team, led by Dr Raquel Alfonso Ballester, together with Dr Norberto Cassinello and Dr Georgy Kadzhaya. Vascular and Hepatic Surgery teams were on standby as a precaution; however, their intervention was ultimately not required, as intraoperative findings confirmed the absence of Inferior Vena Cava infiltration.
Surgical Outcome: Successful Resection of Adrenocortical Carcinoma
The 3D model played a key role in surgical planning, providing confidence regarding the tumour’s relationship with adjacent structures and the extent of vascular involvement.
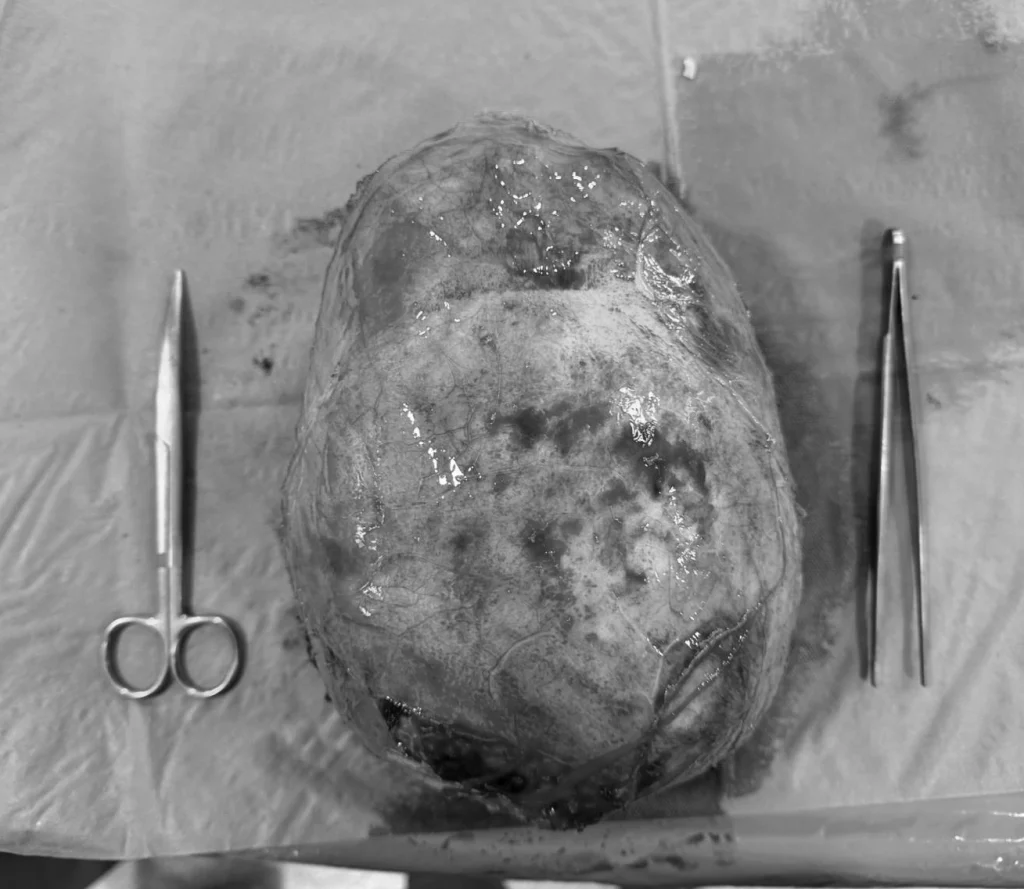

Complete resection of the adrenocortical carcinoma was achieved successfully and without complications, despite tumour contact with the Glisson’s capsule.
¡Follow us on social media to stay up to date with our latest clinical cases and innovations!